COVID-19 Revisitando as vias inflamatórias na artrite
Nat Rev Rheumatol 2020 doi.org/10.1038/s41584-020-0451-z
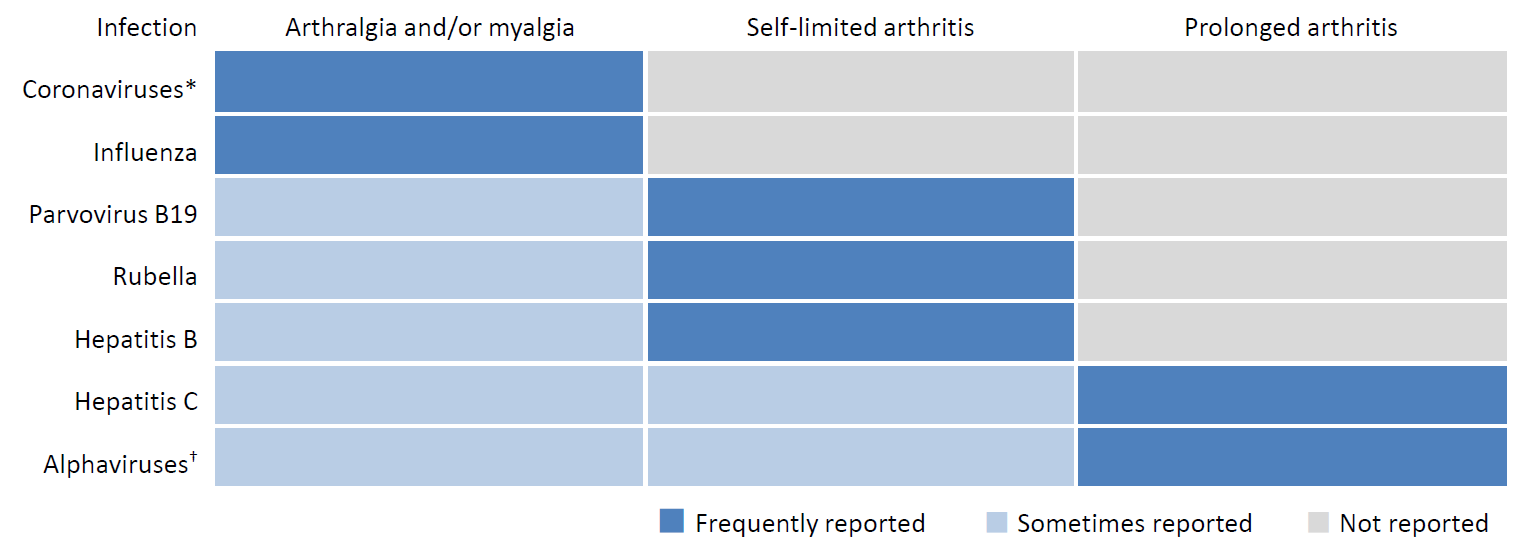
This review investigates the potential implications of COVID-19 on the field of rheumatology. Common pathways in COVID-19 and RA have provided rationale for the trial of DMARD therapies in treatment of severe COVID-19 infections. Safety considerations of RA patients undergoing immunomodulatory treatments are reviewed. Recommendations suggest that RA patients should continue DMARD treatment, whereas glucocorticoid use could be deleterious in COVID-19 infection and should be considered carefully, on a dose by dose basis and pending individual risks. This should now be further considered in terms of the RECOVERY study published in NEJM July 2020 (Horby et al) in which dexamethasone was found to be helpful in a proportion of COVID-19 patients with severe disease.Various rheumatic symptoms have been reported in patients who have contracted viral infections, ranging from arthralgia to chronic arthritis. Arthralgia and/or myalgia is frequently reported in patients with various coronaviruses. Furthermore, studies have suggested those that have contracted coronavirus are at an increased risk of developing RA in the future, even after viral clearance.Severe COVID-19 infection and RA have been noted to share disease mechanisms, including cytokine profiles and cellular processes. Selective cytokine blockade using IL-6R antagonists and IL-6 inhibitors in COVID-19 infection is being trialled alongside studies using JAK inhibitors in severe cases of COVID-19, as are many other cytokine inhibitor pathways. JAK inhibitors are also to be used with caution, due to concerns of leukopenia and impaired interferon-mediated anti-viral responses during treatment – clinical trials are underway to establish whether this is a robust conclusion.Fewer rheumatologists have been in clinic during the pandemic due to absence resulting from disease, quarantine, and involvement in COVID-19 units. This means work reorganisation must be considered to account for a reduced workforce. Postponing non-urgent visits to clinic and weighing potential harm of delaying in person treatments with contracting COVID-19 must be considered. Concerns must also be contemplated regarding a potential shortage of DMARDs due to an increased demand of use in COVID-19 trials and cases.