Evaluation of the Short-, Mid-, and Long-term Effects of Tofacitinib on Lymphocytes in Patients with Rheumatoid Arthritis
van Vollenhoven R,
Lee EB,
Strengholt S,
Mojcik C,
Valdez H,
Krishnaswami S,
Biswas P,
Lazariciu I,
Hazra A,
Clark JD,
Hodge J,
Wang L,
Choy E
Arthritis Rheumatol 2018 DOI: 10. 1002/art.40780
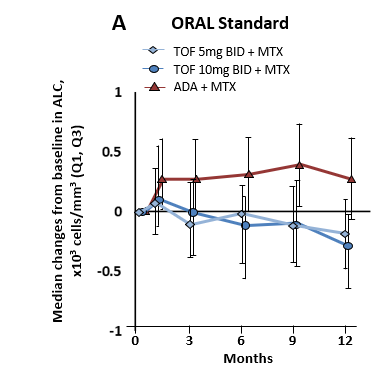
Tofacitinib (TOF) treatment is associated with short-term transient increases in absolute lymphocyte counts (ALC), followed by a gradual decline to reach steady state by ~48 months. Changes in both ALC and lymphocyte subset counts (LSC) were reversible upon TOF discontinuation. Low ALC but not LSC were associated with an increased risk of serious infective episodes (SIEs) and herpes zoster (HZ). This data supported the treatment recommendations on ALC counts for starting and continuing therapy with TOF.Altered lymphocyte counts, and increased infection rates, have been reported in RA patients treated with JAK inhibitors. This study evaluated the short, mid, and long-term effects of TOF on lymphocyte counts and infection rates in RA patients. The reversibility of ALC and LSC changes were also assessed. The value of monitoring ALC alone was assessed by examining ALC/LSC correlations to infections.ALC and LSC data was collected from a variety of the development studies for TOF. An initial increase in ALC was observed, which steadily declined following the first month of treatment reaching steady state at ~48 months. Changes in both ALC and LSC were reversible after treatment cessation with a median time of 3–6 weeks. Low ALC (<500 cell/mm3) was generally associated with an increased risk of SIEs and HZ. There was no strong correlation between LSCs and SI incidences rates. Thus, ALC monitoring alone appears to be adequate to assess infection risk in TOF treated RA patients. Current supporting treatment recommendations suggest TOF initiation is not recommended in patients with ALC <500 cell/mm3. Those developing this during treatment are recommended to temporarily discontinue TOF treatment and restart 5 mg QD with continued monitoring once ALC >500 cell/mm3 has been reached.