Two Years of Sarilumab in Patients with Rheumatoid Arthritis and an Inadequate Response to MTX: Safety, Efficacy and Radiographic Outcomes
Genovese MC,
van Adelsberg J,
Fan C,
Graham NMH,
van Hoogstraten H,
Parrino J,
Mangan EK,
Spindler A,
Huizinga TWJ,
van der Heijde D,
for the EXTEND study investigators
Rheumatology 2018;57:1423–1431 DOI: 10.1093/rheumatology/key121
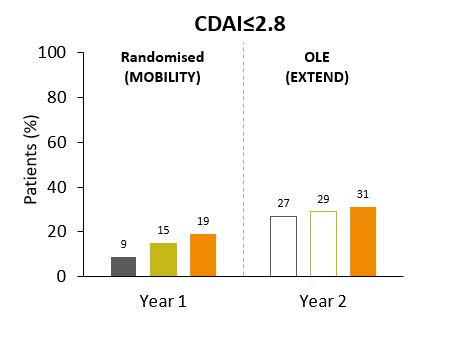
Two-year treatment of active, moderate-to-severe RA with sarilumab, along with dose reduction in the event of laboratory abnormalities, resulted in durable efficacy outcomes and a safety profile consistent with previous reports involving IL-6R inhibition. Durable long-term safety and efficacy, reduced joint damage progression, and conserving health-related quality of life and work productivity are important goals of therapy in RA.1 Sarilumab significantly reduced disease activity, improved physical function and inhibited radiographic progression compared with placebo plus MTX in MOBILITY – a 52-week, double-blind, phase 3 study in patients with active, moderate-to-severe RA and inadequate response to MTX.2EXTEND was an open-label extension (OLE) in which patients who completed MOBILITY continued or were switched to SAR 200 mg Q2W. The study examined the safety and durability of response of SAR 200 mg Q2W, and whether AEs could be managed with dose reduction to SAR 150 mg Q2W. The most common TEAEs were consistent with IL-6R blockade and included neutropenia and injection site erythema. Decreased absolute neutrophil count and increased levels of ALT were the most common reasons for dose reduction, which was required in 14.4% (n=123) of patients. Reducing the dose of sarilumab from 200 to 150mg Q2W allowed 89.4% of these patients (n=110) to continue the study through 2 years. Discontinuation rates were similar across original treatment groups. Clinical responses, including DAS28-CRP, CDAI and HAQ-DI, were also similar irrespective of initial treatment, and radiographic progression measured by modified Sharp-van der Heijde score stabilised.The authors concluded that 2-year treatment of active, moderate-to-severe RA with SAR, along with dose reduction in the event of laboratory abnormalities, resulted in durable efficacy outcomes and a safety profile consistent with previous reports and IL-6R blockade.1. Scott DL, et al. Lancet 2010;376:1084–1108. 2. Genovese MC, et al. Arthritis Rheumatol 2015;67:1424–1437.