Filgotinib Versus Placebo or Adalimumab in Patients with Rheumatoid Arthritis and Inadequate Response to Methotrexate: A Phase III Randomised Clinical Trial
Combe B,
Kivitz A,
Tanaka Y,
van der Heijde D,
Simon JA,
Baraf HSB,
Kumar U,
Matzkies F,
Bartok B,
Ye L,
Guo Y,
Tasset C,
Sundy JS,
Jahreis A,
Genovese MC,
Mozaffarian M,
Landewé RBM,
Bae S-C,
Keystone EC,
Nash P
Ann Rheum Dis. 2021 Jan 27:annrheumdis-2020-219214
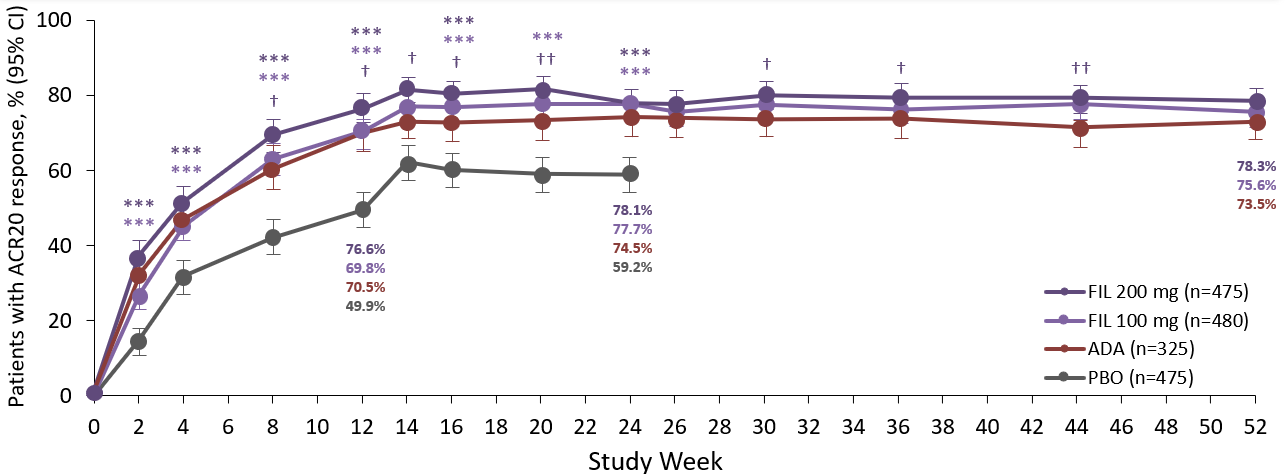
Filgotinib improved RA signs and symptoms, physical function, and inhibited radiographic progression. FIL 200mg plus MTX, but not FIL 100mg plus MTX showed non-inferiority to ADA plus MTX, based on DAS28(CRP) low disease activity. FIL was also well tolerated in RA patients with inadequate response to MTX.This 52-week, phase 3 randomised clinical trial (FINCH 1) evaluated the efficacy and safety of FIL in patients with RA randomised to FIL 200 or 100mg, ADA 40mg, or placebo, all with background MTX treatment. The primary endpoint was the proportion of patients achieving ACR20 at week 12. Additional efficacy outcomes at week 12 included changes from baseline scores for HAQ-DI and DAS28(CRP) <2.6. Safety was also assessed from adverse events and laboratory abnormalities. ACR20 at week 12 was significantly higher for FIL 200 (76.6%) and 100mg (69.8%) vs placebo (49.9%). Improvements at week 12 with FIL vs placebo treatment were also observed in HAQ-DI and DAS28(CRP) <2.6. Radiographic progression of structural join damage was significantly reduced in both FIL dose arms vs placebo at week 24. Although FIL 200mg was non-inferior to ADA at week 12 for DAS28(CRP) ≤3.2, FIL 100mg did not achieve non-inferiority vs ADA. Overall, FIL showed a favourable benefit-to-risk profile and both doses were well tolerated. FIL with background MTX could therefore be considered a treatment option in patients with RA and an inadequate response to MTX.