関節リウマチ患者におけるトファシチニブの減量, 中止, および再 開に関する結果: 前向き観察研究
Clin Rheumatol. 2019 Aug 9. DOI: 10.1007/s10067-019-04721-z
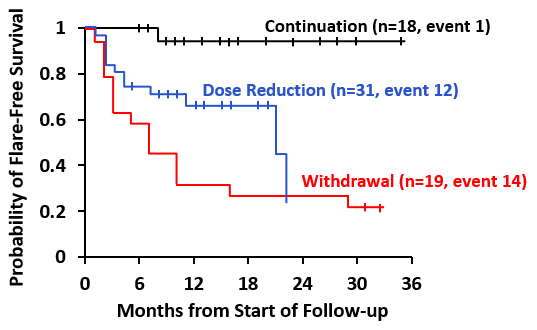
Following achievement of remission or low disease activity (LDA), a dose reduction strategy of TOF to a 5mg QD dose was preferable to immediate withdrawal of TOF, with lower relapse rates.Clinical remission or LDA early in the disease course is a target for every RA patient. Although maintaining a state of remission or LDA is beneficial to patients, the AEs and costs associated with DMARDs, have significant burdens on patients during life-long RA treatment. This long-term study was performed to compare the clinical outcomes of withdrawal, dose reduction and continuation of TOF in RA patients achieving remission or LDA during an induction therapy. All 100 RA patients enrolled into the study was treated with 5 mg TOF BID for one year. Those achieving and maintaining remission at the end of the induction therapy were assigned to withdrawal, dose reduction or continuation groups, who then received periodic follow-up to assess disease activity. In the case of flares, the original treatment regimen was reintroduced. 68 patients during the first year achieved remission or LDA. With a higher crude IR per PY (95% CI) of disease flare in the withdrawal group (0.73), followed by the dose reduction (0.44) and continuation groups (0.04). The withdrawal group also had the lowest median time of flare free survival at 7 months, and 21 months for dose reduction. Adjusted HRs (95% CIs) was similarly higher for withdrawal at 18.11 and lower for dose reduction at 9.13 compared to continuation. Following one year of TOF treatment which induced sustained remission or LDA, the dose reduction strategy seems preferable to immediate withdrawal of TOF. Patients experiencing flares also regained control when restarting the original regimen.