Effects of Baricitinib on Radiographic Progression of Structural Joint Damage at 1 year in Patients with Rheumatoid Arthritis and an Inadequate Response to Conventional Synthetic Disease-modifying Antirheumatic Drugs
van der Heijde D,
Dougados M,
Chen YC,
Greenwald M,
Drescher E,
Klar R,
Xie L,
de la Torre I,
Rooney TP,
Witt SL,
Schlichting DE,
de Bono S,
Emery P
RMD Open. 2018 May 8;4(1):e000662. DOI: 10.1136/rmdopen-2018-000662
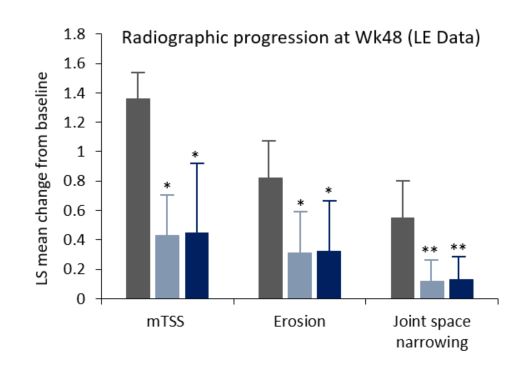
Once daily baricitinib (BARI) inhibited radiographic progression of structural joint damage in patients with an inadequate response or intolerance to csDMARDs over 48 weeks.Current treatment goals aim to use DMARDs to inhibit structural joint damage and prevent long-term functional disability. In RA-BUILD¹, BARI was shown to significantly reduce radiographic joint damage progression in patients with active RA, with an intolerance or inadequate response to csDMARDs. Here, the authors report the long-term radiographic progression of patients enrolled in RA-BEYOND.RA-BEYOND is a long-term extension study of RA-BUILD that evaluated the long-term efficacy and safety of BARI. Of the 611 patients who completed RA-BUILD, 583 patients enrolled into RA-BEYOND. These patients continued to receive the BARI dose (2 or 4 mg QD) they received at the end of RA-BUILD, except placebo patients who were given BARI 4 mg. Radiographic data, including baseline radiographs, mTSS values, bone erosion and joint space narrowing data were obtained over the 48 weeks. Data were analysed using linear extrapolation and last observation carried forward analyses. BARI was shown to inhibit structural damage progression, bone erosion and joint space narrowing in patients with RA at Wk24. These trends were also observed at Wk48, with BARI 4 mg demonstrating significantly less radiographic progression in the observed/last observation carried forward analysis. More patients who received BARI presented no mTSS progression at Wk48, compared with patients given placebo. However, safety analyses showed that from Wk0 to 48, patients given BARI 4 mg reported more treatment-emergent AEs and serious AEs, compared with patients given BARI 2 mg. The authors concluded that both BARI doses were associated with reductions in structural joint damage progression, with the higher BARI dose showing more consistent reductions. Responses observed at 24 weeks in patients given BARI were maintained to 1 year, however, further radiographic assessments need to be completed to determine the longer-term effects of BARI.1. Dougados et al. Ann Rheum Dis 2017; 76:88–95