Long-term Radiographic and Patient-reported Outcomes in Patients with Rheumatoid Arthritis Treated with Tofacitinib: ORAL Start and ORAL Scan Post-hoc Analyses
Strand V,
Kavanaugh A,
Kivitz AJ,
van der Heijde D,
Kwok K,
Akylbekova E,
Soonasra A,
Snyder M,
Connell C,
Bananis E,
Smolen JS
Rheumatol Ther. 2018 Dec;5(2):341-353. doi: 10.1007/s40744-018-0113-7
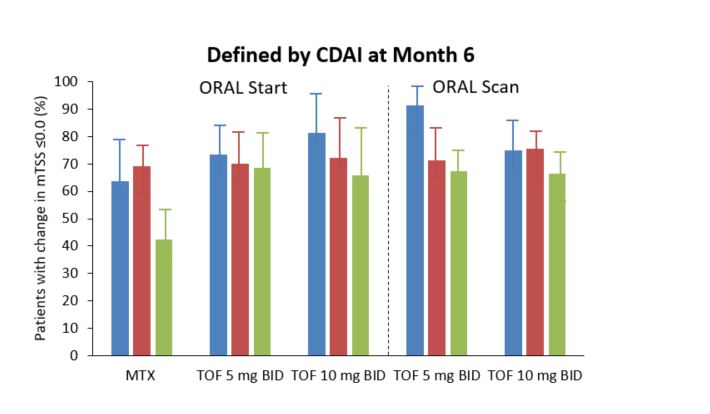
Tofacitinib (TOF) therapy reduced the progression of structural joint damage at 2 years, in patients of all disease states, compared with patients given methotrexate (MTX). Early intervention with DMARDs aim to prevent the development of future RA symptoms and inhibit the progression of structural damage to the joints. This post-hoc analysis uses data from two Phase 3 TOF studies, to examine the efficacy of early intervention with TOF on long-term radiographic outcomes and disease activity states of patients with RA.Data from MTX-naïve patients in ORAL Start¹ and MTX-IR patient in ORAL Scan² were used to assess disease activity at 6 months. Disease activity was measured using CDAI, DAS28-ESR and DAS28-CRP scores, which were then stratified to define each patient’s activity state. Radiographic progression and physical function were analysed by comparing mTSS and HAQ-DI scores, respectively.At 6 months, a higher number of patients given TOF achieved CDAI remission or low disease activity compared with patients given MTX. In these patients, mean change from baseline mTSS was lower compared with patients who had moderate or high disease activity at 6 months. Patients given TOF monotherapy who had CDAI-defined moderate or high disease activity at 6 months, were more likely to show no radiographic progression at 2 years, than patients given MTX. Additionally, patients given TOF who were in CDAI and DAS28-CRP (defined as <1.9) remission reported more normative HAQ-DI scores than patients who achieved the higher remission target of <2.6. Analyses of the data suggested that patient disease activity state at 6 months, was a key indicator for long-term disease progression and improvements in physical function. TOF therapy was shown to be effective in reducing structural joint damage in patients of all disease states, compared with MTX. The authors also suggest that DAS28-CRP<1.9 should be the new remission cut-off in clinical practice, as long-term outcomes achieved in the analyses were similar in patients who achieved CDAI remission and DAS28-CRP<1.9. 1. Lee et al. N Engl J Med 2014 370:2377–86 2. van der Heijde et al. Arthritis Rheum 2013 65:559–70