Inibizione di JAK come Strategia Terapeutica per Patologie Immuni e Infiammatorie
Nat Rev Drug Discov 2017;16:843–62 DOI: 10.1038/nrd.2017.201
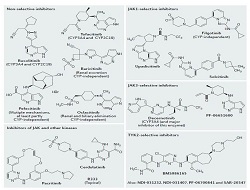
Janus kinases (JAKs) are essential mediators of downstream signaling pathways in many inflammatory and autoimmune diseases. This review summarizes current clinical data on first- and second-generation JAK inhibitors (jakinibs) and discusses their use for the treatment of immune and inflammatory conditions.First generation jakinibs such as tofacitinib, baricitinib, and ruxolitinib, non-selectively inhibit JAK-dependent pro-inflammatory cytokines, which are major contributors to immunopathology. Tofacitinib targets JAK3 and JAK 1, with some activity at JAK2. Based on clinical data from six Phase 3 studies in over 6000 patients, tofacitinib is approved for the treatment of patients with RA. Tofacitinib is also being evaluated for a variety of other diseases including psoriatic arthritis, psoriasis, ulcerative colitis and juvenile idiopathic arthritis. Baricitinib, which inhibits JAK1 and JAK2, is also approved in Europe for the treatment of RA.The safety profile of tofacitinib is the best characterized of the first-generation jakinibs. Adverse effects reported with first-generation agents include infection, anemia and leukopenia, and gastrointestinal perforation. Long-term monitoring is required to determine how JAK inhibition affects the risk of cardiovascular disease and cancer.Second generation jakinibs, with a narrow spectrum of action on cytokines, are in clinical development (e.g. decernotinib, upadacitinib and filgotinib). These agents aim to achieve similar efficacy and improved safety profiles compared with first-generation agents.In summary, first generation non-selective jakinibs (e.g. tofacitinib and baricitinib) are approved for the treatment of patients with RA and have demonstrated efficacy and favorable safety profiles in clinical trials of other immune and inflammatory conditions. Second-generation jakinibs are in clinical development; however, important questions remain about the advantages and limitations of improved JAK selectivity.